Get the facts about breast reconstruction |
Vertical Divider
|
What is a mastectomyA mastectomy is usually carried out to treat breast cancer. In some cases, people believed to be at high risk of breast cancer have the operation prophylactically, that is, as a preventive measure. It is also the medical procedure carried out to remove cancerous tissues. Alternatively, some patients can choose to have a wide local excision, also known as a lumpectomy, an operation in which a small volume of breast tissue containing the tumor and a surrounding margin of healthy tissue is removed to conserve the breast.
Traditionally, in the case of breast cancer, the whole breast was removed. Currently the decision to do the mastectomy is based on various factors, including breast size, number of lesions, biologic aggressiveness of a breast cancer, the availability of adjuvant radiation, and the willingness of the patient to accept higher rates of tumor recurrences after lumpectomy and radiation. Outcome studies comparing mastectomy to lumpectomy with radiation have suggested that routine radical mastectomy surgeries will not always prevent later distant secondary tumors arising from micro-metastases prior to discovery, diagnosis, and operation. |
|
Total mastectomy
Simple mastectomy (or "total mastectomy"): In this procedure, the entire breast tissue is removed, but axillary contents are undisturbed. Patients who undergo simple mastectomy can usually leave the hospital after a brief stay. People that are more likely to have the procedure of a simple or total mastectomy are those that have large areas of ductal carcinoma in situ or even those persons that are removing the breast because of the possibility of breast cancer occurring in the future (prophylactic mastectomies). When this procedure is done on a cancerous breast, it is sometimes also done on the healthy breast to forestall the appearance of cancer there called contralateral prophylactic mastectomy. Partial mastectomy Partial mastectomy is the removal of the cancerous part of the breast tissue and some normal tissue around it. While lumpectomy is technically a form of partial mastectomy, more tissue is removed in partial mastectomy than in lumpectomy. Prophylactic mastectomy This procedure is used as a preventative measure against breast cancer. The surgery is aimed to remove all breast tissue that could potentially develop into breast cancer. Prophylactic mastectomy is generally considered when the patient has BRCA1 or BRCA2 mutations in their genes. |
Contralateral prophylactic mastectomy
This procedure removes the non cancerous breast and breast tissue. Skin sparing In this surgery, the breast tissue is removed through a conservative incision made around the areola (the dark part surrounding the nipple). The increased amount of skin preserved as compared to traditional mastectomy resections serves to facilitate reconstruction procedures. Some patients who have a reduction in skin pocket will have additional scars. Patients with cancers that involve the skin, such as inflammatory cancer, are not candidates for skin-sparing mastectomy. Nipple sparing Breast tissue is removed, but the nipple-areola complex is preserved. This is the treatment of choice for prophylactic cases, for mastectomy for benign disease or if the cancer is a considerable distance away from the nipple-areolar complex. If the cancer is close to the nipple-areolar complex then this method of mastectomy is not recommended due to fears of increased cancer development in retained areolar ductal tissue. |
What will I do about my breast? section by Professor John Boyages
The absolute medical reasons to have a mastectomy are:
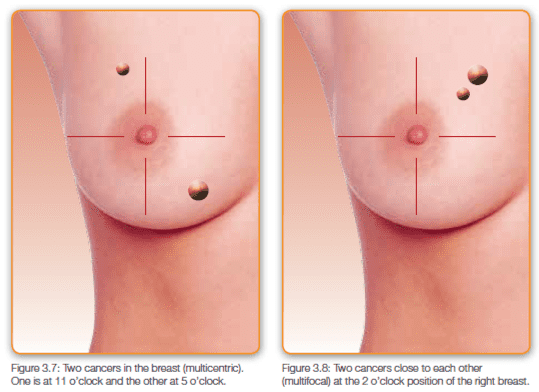
- When there is more than one cancer in different quadrants of the breast. If there is a cancer, for example, at the 11 o’clock position, 50 mm (2 inches) above the nipple; and another at the 5 o’clock position, 80 mm (3 inches) below the nipple, then you are probably better off having a mastectomy. This situation is called multicentric cancer (Figure 3.7). On the other hand, if you have two or more cancers in the same quadrant that are quite close together and can still be removed with a clear margin, then there is absolutely no need to have a mastectomy. This situation is called multifocal cancer (Figure 3.8).
- If, as a child or a teenager, you had cancer that required radiation therapy. Some patients with a type of cancer of the lymph glands known as Hodgkin’s lymphoma will have had radiation therapy in the past to the breast area that may make subsequent radiation therapy to the breast quite difficult.
- If you have a very large cancer particularly in a smaller breast
- If you just feel more comfortable having a mastectomy than going through five or six weeks of radiation
- If you are pregnant, you cannot receive radiation until you have delivered your baby, so a mastectomy may be more appropriate for you
- Some pre-existing diseases (such as severe scleroderma or rheumatic diseases requiring high-dose steroids) may make you more prone to radiation complications, and a mastectomy may be less complicated
- If clear margins cannot be obtained after one or two breast conserving procedures.
Having a strong family history of breast cancer is not necessarily an indication for a mastectomy. Some doctors do occasionally recommend removing both breasts in this setting, but there is no consistent evidence that this increases your chance of surviving breast cancer (Recht 2009). Recht recently noted that some caregivers recommend a mastectomy for patients with strong family histories of breast cancer, or with a BRCA1 or 2 defect or mutation, because they feel that breast conservation is not effective in this group. He notes that this recommendation lowers the psychological barrier to removal of the normal breast. This has resulted, without strong research evidence, in removing both breasts for patients with strong family histories. However, he reports that most studies have found little or no difference in the chance of cancer coming back after breast conservation for patients with or without the breast cancer gene.
The difference between a breast surgeon and a general surgeon
Surgeons are always trained first as general surgeons, and then they usually specialize in a field such as brain, heart, or breast surgery, particularly if they work in a large hospital or academic university hospital. If you can, consult a breast surgeon who sees and treats breast cancer every single day. Take care if your surgeon spends a lot of his or her week doing gallbladders, hemorrhoids, varicose veins, or colorectal cancer and only operates on the occasional patient with breast cancer.
Ask your surgeon, “Do you treat conditions other than breast cancer—just in case we need you for something else?” It’s a bit of a trick question, but this is a polite way of trying to work out if he or she is a general surgeon rather than a “breast surgeon.” I do, however, exclude very experienced rural surgeons. It’s impossible for every country town or small state to have a breast surgeon. My experience of these country surgeons is that they provide an exceptional service and work very hard to keep up to date and link in with experienced breast surgeons by telephone, e-mail, or video conference.
Remember that an experienced general car mechanic in the country may still be better than the young Ford mechanic in the city. You can ask the surgeon, “What proportion of your work is breast disease?” Remember that very busy breast surgeons may focus 80–90 percent of their practice on breast disease and 10 percent on hormone conditions such as thyroid disease. Some surgeons sub-specialize in cancer operations (surgical oncologist), and some may focus on both breast cancer and melanoma (a type of skin cancer). Breast surgeons know about sentinel node mapping and the sentinel node biopsy technique, explained in the next chapter, and generally work in a team that includes at least a radiation oncologist and a medical oncologist.
What is oncoplastic surgery?
Some surgeons are now trained in advanced plastic surgery techniques to reshape the remaining breast after your cancer is removed. This is sometimes referred to as oncoplastic surgery. The breast surgeon uses plastic surgical techniques in order to reshape the remaining healthy breast or reconstruct the affected breast after removal of DCIS or breast cancer. It also includes the correction of any imbalance relative to your healthy breast. Oncoplastic surgery is ideal for some women who not only have to deal with the diagnosis but also the effect of possible disfiguring surgery to their breast. Oncoplastic surgery may include the following:
With breast conservation
- Removing the breast cancer with a clear margin
- Using small scars with dissolving stitches under the skin
- The displacement of nearby breast tissue into the defect which is left when your cancer and surrounding healthy tissue is removed
- The use of breast reduction techniques in order to refashion the whole breast after your cancer is excised with reduction of the other side to achieve symmetry (Figure 3.13). Your surgeon may place a clip made from titanium where your cancer started so we know where to give a higher dose of radiation (see “boost” in Control Point #14 –Do I Need Radiation Therapy?” I have seen a few patients with reduced nipple sensation on both sides after bilateral breast reducing surgery and removal of her cancer on the affected side. Make sure you check with your surgeon about their own experience with this type of surgery (Figure 3.13).
- The replacement of tissue into the surgical defect by moving muscle and skin tissue from elsewhere, for example the Latissimus dorsi muscle (LD) flap (see Control Point #6 – If I Have a Mastectomy, What Are My Options for Breast Reconstruction?).
With a mastectomy:
- Removing all of your breast which leaves behind the skin and some underlying fat and an immediate sub-pectoral tissue expander or muscle flap (see Control Point #6 – If I Have a Mastectomy, What Are My Options for Breast Reconstruction?). In this option the skin and nipple areola is removed from the central part of your breast (with the underlying breast tissue).
- Having a “skin-sparing mastectomy” where the breast tissue and the nipple and areola are removed through a small scar and less of the overlying skin is removed. The breast mound is then recreated and the natural shape and contour of the breast is preserved, using either a permanent implant or tissue flap (Patani, 2008).
- As for a skin-sparing mastectomy, but with preservation of the nipple and areola (“ nipple-sparing mastectomy”) without removal of skin and without an enhancement of the other side.
Skin-sparing mastectomy
The skin-sparing mastectomy was first described over 20 years ago in an effort to maximize preservation of the skin of the breast after a mastectomy, to improve the cosmetic appearance of the breast and to make breast reconstruction easier by having more tissue to work with (Toth 1991). It typically involves removal of the entire breast and nipple-areola complex while preserving the skin envelope and the natural curvature under your breast (the inframammary fold).
Because less skin is removed, research has been done which looked at the chance of finding residual breast tissue or even disease under the skin that is left behind after a skin-sparing mastectomy. In one study, the chance of finding residual breast tissue was almost 60% and residual disease was left behind in 10% (Torresan 2005). Despite this, with well-selected patients the chance of a recurrence after a skin-sparing mastectomy is very low. In a review article, Tokin (2012) reported on five studies involving 368 patients, of whom four patients recurred (1.1%). Most of these studies had short observation periods of less than 5 years. This rate is likely to go up a little with time.
Usually after a skin-sparing mastectomy, because of the amount of skin left behind (the so called “skin-envelope”), reconstruction needs to take place either with an expander followed by a silicone implant at a later date or an immediate silicone implant. Or, for some patients with larger breasts, a flap with some normal skin and muscle tissue can be used (see Control Point # 6 What are my Options for Breast Reconstruction?”). A variant of a skin-sparing mastectomy is a “skin-reducing mastectomy” used for larger breasted women which is like a combination of a breast reduction and a reconstruction with an immediate implant.
Radiation therapy may still be indicated after these types of procedures and this may cause some thickening around your implant and some asymmetry. The indications for post-mastectomy radiation are discussed in Control Point #14 Do I Need Radiation Therapy?
Complications after a skin-sparing mastectomy include infection, other wound complications or loss of the implant. There is a higher risk of delayed wound healing with skin-reducing mastectomy than with other mastectomy types because the blood supply needs to be distributed to a larger portion of skin. For the standard skin- or nipple-sparing mastectomy, wound healing is usually not a problem, because, in fact, the incisions used are smaller than that of a standard mastectomy. Implant loss has been reported to be on average around 14% (Kobraei 2012).
Nipple-sparing mastectomy
Nipple-sparing mastectomy is a variety of skin-sparing mastectomy where the entire skin of the breast is preserved, including the nipple-areola complex. This is the procedure some women with a very strong family history of breast cancer, like Anjelina Jolie, have done to prevent the onset of breast cancer.
The ducts inside of the nipple (its “core”) are usually removed. Nipple-sparing mastectomy is particularly suitable for women with smaller breasts and often the other breast is enlarged with an implant at the same time (Figure 3.15). This is still possible with larger breasted women, but nipple-sparing mastectomy has been considered safe for women with small, solitary tumours located away from the nipple or when a mastectomy is done as a preventative measure. Some women may have a skin-sparing mastectomy on the side of their cancer and, because of an increased risk on the other side, due for example to a strong family history, may have a nipple-sparing mastectomy on the healthy side to reduce their future risk of cancer developing. For other women, they may choose to have any decisions about the other side deferred until all their other treatments such as chemotherapy and radiotherapy are completed (Figure 3.16).
A review paper about nipple-sparing mastectomy examined all the publications which studied nipple involvement for women who had undergone a mastectomy (Rusby 2010). The authors found that 13 studies contained a minimum of 100 patients per study and over 4500 total patients. The average incidence of nipple involvement was 14% (range, 6-31%). These studies are not all alike and vary by not only the type of patients who were included (ranging from early to more advanced disease) but also the pathology technique use to examine the nipple.
If you are keen to try this remember that if the nipple is involved there is still the option of going back and having a second anesthetic to remove the nipple and areola region. One large group from the US initially recommended a nipple-sparing mastectomy only after a pre-operative breast MRI showed no abnormality within 2cm of the nipple (Wijayanayagam 2008). However, as their experience evolved, they now only use an MRI in cases where the tumour is close to the nipple on clinical examination or mammography; if preoperative MRI demonstrates no clear tumour involvement of the nipple or areola, patients are still eligible for this technique, even if the tumour lies within 1cm of the nipple region (Peled 2012). This study, led by Laura Esserman, found that the tissue and ducts behind the nipple had disease present in only 3 out of every 100 patients (3%).
Another drawback of this technique is the chance of the nipple losing its blood supply and dying off (“necrosis”). It is likely that the risk is higher if you continue to smoke or if you are older or have vascular disease all of which can affect the blood supply and healing. Some researchers have found that nipple necrosis was more common when an incision was made centrally around the areola (periareolar incision) compared to a scar in the outer half of the breast (Regolo 2008). Others have found that using an expander (which slowly stretches the skin and nipple) rather than a permanent fixed volume implant improved nipple survival (Peled 2012).
In the review article, Tokin (2012) reported on 14 studies involving 2406 patients treated with a nipple-sparing mastectomy. Out of the 2406 patients, 257 (10.7%) developed some or total loss of the nipple. In total, 66 patients (2.7%) lost their entire nipple due to it dying off from a lack of blood supply, but there were lower rates of complications from different surgical approaches and techniques. Ask your surgeon about what his or her rates of nipple necrosis are and how many they have done.
In Laura Esserman’s study, once their technique was refined, nipple necrosis occurred in 2 out of every 100 patients (one complete and one partial) (1.8%), and necrosis of the overlying mastectomy skin occurred in 11 patients out of every 100 (11.3%). Complications requiring removal of the implant occurred in 8 out of every 100 women (8.4%) (Peled 2012).
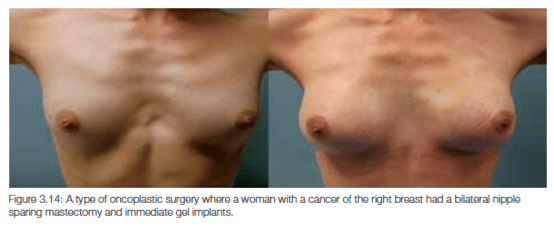
Normal nipple sensitivity is very unusual after these procedures. Some sensation in the surrounding skin may be possible in many women and only a few nipples remain potentially erectile. The cosmetic results from a nipple-sparing mastectomy can be excellent (Figure 3.14) but you may appear unbalanced if some sort of lift is not done on the other side.
Radiation to the skin of your new breast may be required and this can tighten your skin a little causing more asymmetry. I have seen a few patients with disastrous cosmetic results from surgeons who really didn’t have the expertise to do this type of procedure. If you are considering this type of surgery, make sure you see a surgeon who has a lot of experience in this technique and, importantly, works in a multidisciplinary team. If your case is complicated, for whatever reason, it’s often worthwhile seeing other team members such as a plastic surgeon, breast care nurse, radiation oncologist and psychologist before your surgery. Remember, it’s not an emergency so you have time to reach the right decision for you.
So, it’s not that straightforward, and expertise for these types of operations vary. What is needed is a very careful discussion with a breast and/or a reconstructive surgeon to determine your potential to have one of these more advanced potentially one-stage procedures. Broadly speaking, the surgeons I work with consider the ideal patient to be one who does not have any oncological contraindication to a nipple-sparing mastectomy such as advanced cancer with skin involvement or disease very close to the nipple. This ideal patient would be a non -smoker, non-diabetic, unlikely to require post-mastectomy radiation with no underlying chronic disorders (such as diabetes or rheumatoid arthritis), be no greater than a C-cup breast and who after full consent understands and is prepared to accept all the potential risks and complications associated with implant based reconstruction. These operations also cost more.
Basically, what you are having with these new type of surgical approaches is a mastectomy—you still lose your entire breast, but you will lose less skin and sometimes keep the nipple.
In the review article, Tokin (2012) reported on 14 studies involving 2406 patients treated with a nipple-sparing mastectomy. Out of the 2406 patients, 257 (10.7%) developed some or total loss of the nipple. In total, 66 patients (2.7%) lost their entire nipple due to it dying off from a lack of blood supply, but there were lower rates of complications from different surgical approaches and techniques. Ask your surgeon about what his or her rates of nipple necrosis are and how many they have done.
In Laura Esserman’s study, once their technique was refined, nipple necrosis occurred in 2 out of every 100 patients (one complete and one partial) (1.8%), and necrosis of the overlying mastectomy skin occurred in 11 patients out of every 100 (11.3%). Complications requiring removal of the implant occurred in 8 out of every 100 women (8.4%) (Peled 2012).
Normal nipple sensitivity is very unusual after these procedures. Some sensation in the surrounding skin may be possible in many women and only a few nipples remain potentially erectile. The cosmetic results from a nipple-sparing mastectomy can be excellent (Figure 3.14) but you may appear unbalanced if some sort of lift is not done on the other side.
Radiation to the skin of your new breast may be required and this can tighten your skin a little causing more asymmetry. I have seen a few patients with disastrous cosmetic results from surgeons who really didn’t have the expertise to do this type of procedure. If you are considering this type of surgery, make sure you see a surgeon who has a lot of experience in this technique and, importantly, works in a multidisciplinary team. If your case is complicated, for whatever reason, it’s often worthwhile seeing other team members such as a plastic surgeon, breast care nurse, radiation oncologist and psychologist before your surgery. Remember, it’s not an emergency so you have time to reach the right decision for you.
So, it’s not that straightforward, and expertise for these types of operations vary. What is needed is a very careful discussion with a breast and/or a reconstructive surgeon to determine your potential to have one of these more advanced potentially one-stage procedures. Broadly speaking, the surgeons I work with consider the ideal patient to be one who does not have any oncological contraindication to a nipple-sparing mastectomy such as advanced cancer with skin involvement or disease very close to the nipple. This ideal patient would be a non -smoker, non-diabetic, unlikely to require post-mastectomy radiation with no underlying chronic disorders (such as diabetes or rheumatoid arthritis), be no greater than a C-cup breast and who after full consent understands and is prepared to accept all the potential risks and complications associated with implant based reconstruction. These operations also cost more.
Basically, what you are having with these new type of surgical approaches is a mastectomy—you still lose your entire breast, but you will lose less skin and sometimes keep the nipple.
Excerpts from Breast Cancer: Taking Control by Professor John Boyages - Read more
(Copyright BC Publishing with permission; www.bcpublish.com)
(Copyright BC Publishing with permission; www.bcpublish.com)


